Healthcare
Ecosystem Constitution & Architecture
A governed healthcare operating ecosystem for coherence, continuity, and system-wide coordination
Most healthcare environments are not true systems. They are partially synchronized subsystems operating through local logic, fragmented state interpretation, and human compensation. This project proposes a different architecture: a governed healthcare ecosystem in which coordination, continuity, access, capacity, and systemic integrity are structurally organized through a central core and a set of specialized but non-autonomous subsystems.
What is
The deepest problem in modern healthcare is not simply missing technology, missing effort, or missing regulation. It is structural fragmentation. Most healthcare infrastructures operate through locally optimized modules that are only partially synchronized, without a continuous shared state space, unified capacity awareness, or full continuity across the patient journey.
This creates repeated actions, duplicated administration, overlapping data, discontinuous interpretation, and unnecessary loss of time and human energy. The same information is often requested multiple times, entered in different places, reconstructed across disconnected contexts, and carried forward through human workaround behavior that should not be necessary in the first place.
The problem is systemic in its effects, but structural in its origin. Its consequences propagate across the whole environment – delays, overload, blind spots, duplicated effort, fragmented continuity – because the architecture itself does not allow the system to perceive and coordinate as one coherent organism.
Fragmented decision spaces
Repeated actions
Duplicated data
No state continuity
What this architecture actually is
This project is a federated, zero-trust healthcare operating ecosystem.
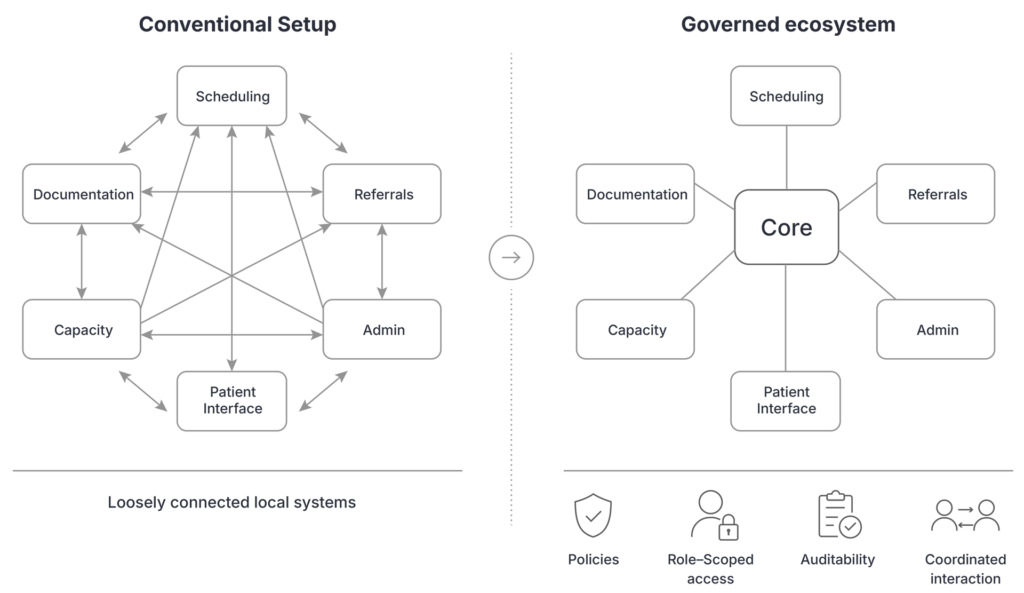
It is not built on implicit trust between subsystems, not on unrestricted data sharing, and not on monolithic storage. It is built on governed interaction, explicit policy, role-scoped access, mediated coordination, and auditability.
Its function is not to replace clinical judgment, but to create the structural conditions under which:
- system-wide coordination becomes possible
- continuity can be preserved
- capacity can be interpreted coherently
- and professionals are relieved from compensating for structural blind spots.
Why healthcare
must be organized around the patient’s state trajectory
A patient does not experience healthcare as separate modules, departments, or transactions. A patient moves through changing physical, cognitive, emotional, behavioral, and clinical states over time. If the system is not organized around this evolving trajectory, continuity breaks, interpretation fragments, and intervention logic becomes inconsistent.
This is why the patient’s state trajectory must become the primary organizing principle of the ecosystem. Referral, triage, scheduling, diagnostics, treatment, medication, nutrition, follow-up, and patient-side interaction are not separate digital functions. They are coordinated transformations within one continuous system reality.
A coherent healthcare architecture should therefore follow the person, not the institution; the evolving state, not the isolated event; the trajectory, not the transaction.

Prevention

Symptoms
Diagnosis
Treatment

Follow Up

Long–term management
Not just an ecosystem –
an operating organism
This architecture is not simply a set of healthcare functions connected under one umbrella. It is a governed system of systems designed to behave as an organism-like coordination environment: a living architecture in which state, response, capacity, decision support, and continuity are structurally interdependent.
In an organism, the parts do not merely coexist. They continuously inform, regulate, and adapt to one another. Healthcare systems need the same operating logic if they are to function systemically rather than administratively. Unexpected events should not create collapse and manual firefighting. They should trigger recalibration.
This is why the architecture is closer to physiology than to conventional software integration. It is not built to connect modules after the fact. It is built to sustain coherence across a living field of interdependent states.
How the ecosystem works
The ecosystem works by creating continuity around the patient’s evolving state and aligning the surrounding system around that continuity. Instead of fragmented interventions, it enables coordinated systemic response across time, function, and role.
State recognition
The system identifies the relevant patient state and its immediate context.
Trajectory interpretation
The current state is interpreted as part of a broader patient trajectory, not as an isolated event.
Coordinated response logic
Scheduling, care, administration, documentation, and support functions align around the same evolving state reality.
Shared continuity
Relevant actors work from connected state visibility instead of disconnected local snapshots.
Adaptive adjustment
As conditions change, the ecosystem recalibrates rather than forcing manual workarounds.
Structural learning
The system accumulates mapped knowledge from recurring transitions, coordination patterns, and pathway outcomes.
Core operating principles
This ecosystem is built around a small number of non-negotiable structural principles:
Shared state space
instead of synchronized informational fragments
State continuity
instead of episodic, isolated interpretations
Patient trajectory primacy
instead of transaction-centric system logic
Unified capacity field
instead of channel-based load illusions
Cross-system impact awareness
before local optimization
Shared temporal coordination
across actors, timelines, and service conditions
Represented interdependence
instead of hidden downstream effects
Core operating principles
This ecosystem is built around a small number of non-negotiable structural principles:
Shared state space
instead of synchronized informational fragments
State continuity
instead of episodic, isolated interpretations
Patient trajectory primacy
instead of transaction-centric system logic
Unified capacity field
instead of channel-based load illusions
Cross-system impact awareness
before local optimization
Shared temporal coordination
across actors, timelines, and service conditions
Represented interdependence
instead of hidden downstream effects
The role
of the Coordinative Core
At the center of the architecture is a Coordinative Core — not a monolithic database, not a clinical authority, and not a system that decides in place of professionals. Its role is to mediate communication, validate state transitions, enforce policy, preserve auditability, and maintain systemic coherence across all participating subsystems.
Subsystems do not form direct operational dependencies on one another. They interact through the core. This preserves integrity, reduces hidden coupling, and allows the ecosystem to behave as one coordinated environment rather than as a fragile network of bilateral integrations.
The core does not replace human judgment. It stabilizes the conditions under which good human judgment remains possible.

System Architecture:
This ecosystem is not a single platform. It is a system of systems.
Each subsystem remains specialized, but none is allowed to become ecosystem-sovereign. Each performs a distinct role, while the Core preserves coherence across the whole.
Data & Identity Layer
- Patient Data Domain
- Professional Data Domain
- Identity / Consent / Vault / Audit
Operational Systems
- Patient Journey System
- Orders & Tasks Engine
- Resource & Capacity System
- Scheduling & Waitlist System
- Clinical Documentation System
- Medication & Nutrition System
- Safety / Compliance / Audit
- Integration Layer
Capacity, Scheduling, and Professional Coordination
One of the strongest structural differences in this architecture is that time, capacity, specialist availability, equipment access, and operational feasibility are not treated as separate planning surfaces.
Scheduling is not just calendar assignment. Capacity is not just available slots. Specialist presence is not just a timetable. These must be interpreted as one coupled field.
A specialist appointment, a surgery, a diagnostic step, a room, and an equipment slot do not exist independently. Their feasibility must be coordinated together.
Relational knowledge space
Beyond coordination, the architecture includes a relational Knowledge Space.
Its function is not to retrieve isolated answers, rank pre-defined options, or force early resolution. It is designed to construct a weighted relational problem space in which distributed knowledge fragments can be traced, connected, and stabilized around a given origin or problem cluster.
Starting from an initial problem, case abstraction, or exploratory origin, the system derives reference points and builds a relational space around them. From there, it traces possible connections across heterogeneous and historically fragmented knowledge sources — including case studies, publications, observations, failed attempts, descriptions, and research results that may never have coexisted in the same temporal or disciplinary frame.
The outcome is not necessarily an answer. It is a stabilized relational image of the problem space — one that allows human reasoning to proceed within a more explicit, less distorted, and more structurally coherent field.
weighted relational problem exploration
cross-time and cross-context tracing
hidden parallels and partial solution chains
stabilization without premature closure
What this makes possible
This architecture makes possible a different kind of healthcare system:
Continuity
Stronger continuity across the full patient journey.
Fewer state breaks between handoffs, departments, and care phases.
Coherence
More coherent coordination across the wider system.
One governed operational reality instead of loosely synchronized local fragments.
Lower burden
Lower administrative and coordination burden on professionals.
Less repeated entry, repeated clarification, repeated checking, and manual workaround.
Adaptive flow
More adaptive capacity management and service flow.
Resource changes, overload, and disruption handled as system events rather than local chaos.
Better context
Clearer decision context under complexity.
Stronger visibility into what is known, what is missing, and what remains uncertain.
Patient clarity
More coherent patient-side interaction.
Clearer status, next steps, and communication across the care journey.
Long-term transformation
A structural foundation for long-term transformation rather than patch-based digitalization.
New tools and intelligence layers can connect without reproducing the same fragmentation.
Explore the architecture in more depth
This page presents the core logic of the healthcare ecosystem. For a deeper overview of the structural model, architectural principles, and system-level implications, download the case study.